
Vancomycin has a narrow therapeutic index - subtherapeutic exposure is associated with treatment failure and supratherapeutic exposure is linked to acute kidney injury. We experimented with one small nudge in the InsightRX Nova precision dosing software. Across 34 sites that opted in, AUC24 target attainment improved by 1.4%, while no significant improvements were observed at 34 other sites that didn't.
What we changed
Early vancomycin area-under-the-curve over 24 hours (AUC24) target attainment is crucial for treatment efficacy in vancomycin, commonly associated with better patient outcomes. AUC24 24-48 hours out from the dosing decision time is sometimes low for patients who accumulate vancomycin slowly. To help bring this to our clinical user's attention, we suggested adding the AUC24-48 metric to the dosing advice table, like this:
| Dose | Interval | Infusion Length | AUC24-48 | AUC24,ss |
| 750mg | 12 hours | 1 hour | 340 mg·h/L | 402 mg·h/L |
| 1000mg | 12 hours | 1 hour | 378 mg·h/L | 455 mg·h/L |
| 1250mg | 12 hours | 1 hour | 410 mg·h/L | 503 mg·h/L |
Table 1. How the dosing advice table for vancomycin looks if you have this feature on!
Imagine you are the clinician. When you see this metric, you'll see how AUC is ramping up from one day out (AUC24-48) up to steady state (AUC24, SS). This helps you figure out if you want to change the recommended dose to get to the AUC target of 400-600 mg·h/L quickly and safely.
How “ITS” evaluated
Thanks to the thirty-four hospital systems that made this change with us, we can look at what happened with an interrupted time series (ITS) analysis.
ITS is a quasi-experimental method that aims to isolate the impact of a specific intervention in real-world data while other things are also changing. An ITS asks: if we draw a line through the pre-intervention data, and then a line through the post-intervention data, is there a big jump at the intervention point? And do the slopes of the pre- and post-intervention data change? We have previously used an ITS to see how the choice of popPK model impacts patient exposure. We found that another change (switching the default dosing model) improved vancomycin AUC24 target attainment while holding adverse events steady.
We looked at changes in AUC target attainment in the year before and the year after sites added this new column. As a control, we matched these 34 intervention sites with 34 sites that did not implement the new column. The interventions ranged from April 2024 to September 2025. Because there is no intervention date for the control sites by definition, we used the average intervention date of July 1, 2024 as a control.
Did it actually work?
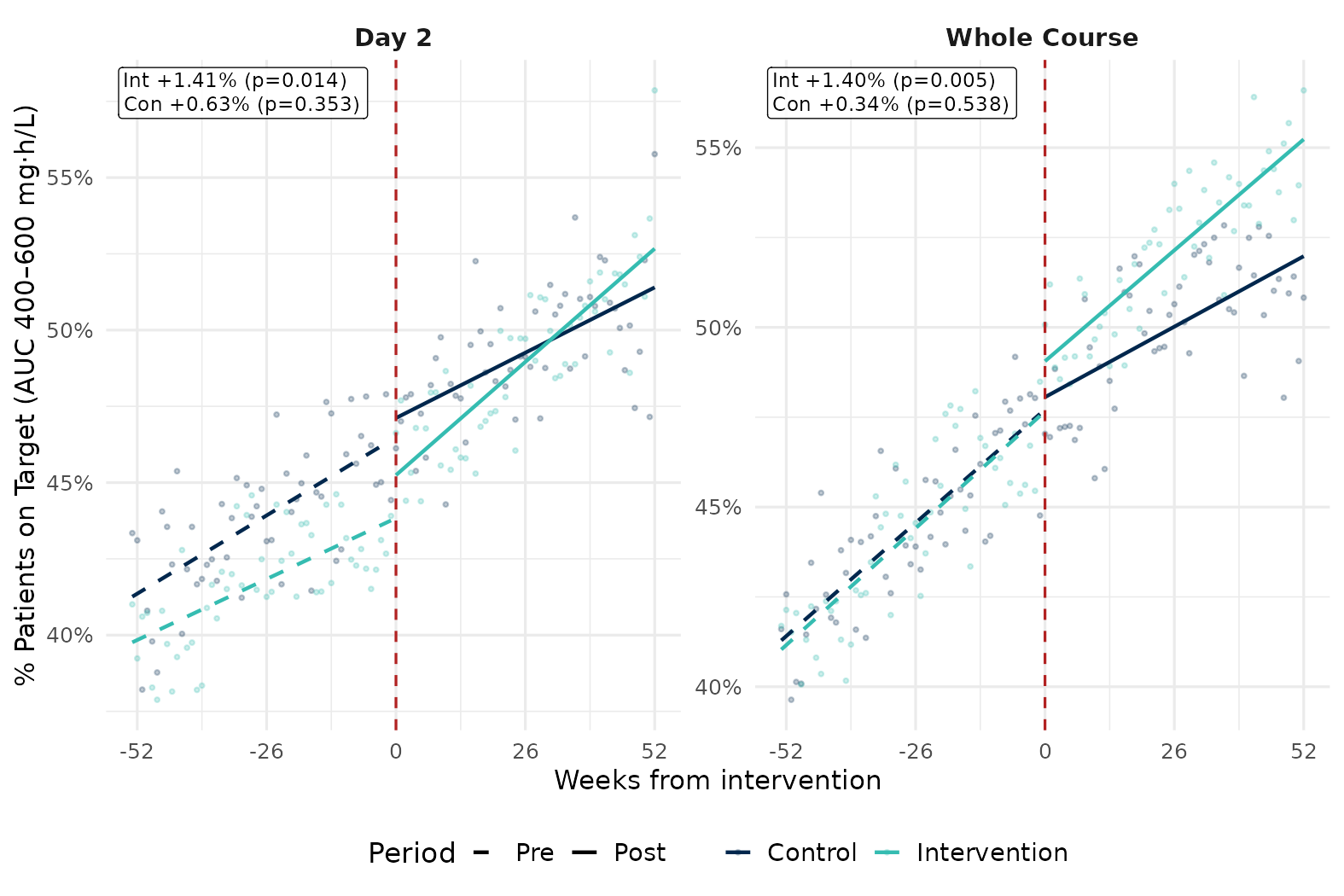
Adding the AUC24-48 metric improved AUC target attainment on day 2 of the treatment course by 1.41% (p = 0.014) and over the whole treatment course by 1.40% (p = 0.005). The control group saw no statistically significant jump in AUC target attainment (AUC day 2: +0.63%, p = 0.353; AUC over the whole treatment course: +0.34%, p = 0.538). While 1.4% seems small, this was also a very small change to the InsightRX Nova software – just adding a column! – and you get one additional patient reaching the target for every 71 patients dosed.

Figure 1. Interrupted time series analysis of vancomycin AUC target attainment on day 2 of the treatment course (left) and over the whole treatment course (right) for 34 hospital systems with the AUC24-48 column turned on at week 0 (teal, intervention group) and 34 systems who did not (navy blue, control group).
What this means for you: one column, 1.4% better target attainment across 34 hospital systems. For a 1000-bed hospital, that's 98 more patients on target per year, (assuming roughly 7 patients/bed/year).
Learn about how hospitals and health systems like yours are using InsightRX to improve care at their organizations.
