When it comes to medications with narrow therapeutic indices, precision is paramount. Recently, the approach to dosing and monitoring vancomycin has shifted towards the use of the area under the concentration-time curve (AUC) as a more accurate measure of drug exposure. However, AUC monitoring brings with it several complexities for calculation and the potential to increase burden on clinicians who are monitoring these patients. To address this challenge, several software tools and various AUC estimation methods are now available to choose from.
Why the Shift to AUC Monitoring?
Traditionally, vancomycin dosing was guided by monitoring trough levels, measured just before the next dose. The most recent update to the vancomycin guidelines, however, supports the use of AUC as a better predictor of toxicity. This is because dosing based solely on trough levels can leads to overdosing and potential toxicity, due to the significant variability in vancomycin pharmacokinetics among patients. AUC monitoring offers a more comprehensive understanding of drug exposure over time, and was always the true pharmacokinetic/pharmacodynamic (PK/PD) target, with trough levels merely acting as a historical surrogate. The change towards AUC-based monitoring aims to optimize therapeutic outcomes while minimizing the risk of toxicity.
Evidence for the benefits of AUC-guided dosing has grown over many years (Brown 2012, Holmes 2013, Jung 2014, Lodise 2014). Operationalizing this switch to AUC-based monitoring, however, has historically been challenging. A number of variables including cost, ease of implementation, and stakeholder buy-in have stymied this switch. To add to the difficulty of decision-making, there are a number of ways to approach measuring & estimating vancomycin AUC – each with its own set of pros and cons.
Click on the following links to jump right into each estimation method:
Two-Level Trapezoidal Method
The trapezoidal rule, a straightforward equation-based method, divides the time-concentration curve into trapezoids and calculates the area under these segments using first-order PK equations.
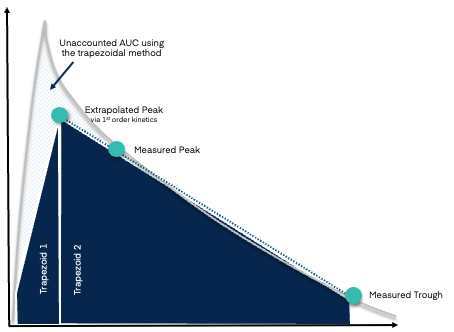
This method relies on drug concentration samples taken at specific time points (i.e. a peak and trough) while at steady-state exposure. Once resulted, these concentration values can then be plugged into static PK equations, either by manual calculation, an Excel calculator, or via an online calculator, to estimate AUC during the infusion and post-infusion period.
| ✅ Pros | ⛔ Cons |
|---|---|
|
Low/No-Costs: Use of this calculation method does not require additional software costs or significant time to implement. |
Limited Calculation Context: Outputs are effectively a snapshot of the patient’s exposure in the sampled interval and are therefore limited in their ability to account for changes in patient status over time, such as renal function or weight – both of which are very important to consider over treatment courses spanning more than a day or two. |
|
Ease of Implementation: Equations can be wrenched into a home-grown calculator, or otherwise easily accessed, for ease of calculation. |
Over-simplified: The trapezoidal method assumes simple one-compartment pharmacokinetics, but vancomycin is largely believed to follow two-compartment pharmacokinetics; this simplification is known to result in underestimation of exposure when using the trapezoidal method. |
|
Familiarity: Conceptually, this approach is relatively easy to introduce and teach as most pharmacists have been exposed to first-order PK equations in their formal education. |
Increased Sampling Burden: Use of the trapezoidal method necessitates more frequent lab draws, further complicated by specific timing requirements:
These specifications will likely raise costs and impact the workflow of phlebotomy and nursing staff. |
|
Error-prone: Vulnerable to errors with manual entry. |
One-level AUC Method
Without the use of Bayesian applications, there has been some discussion about use of a single level to calculate AUC. One-level vancomycin AUC estimations can be performed by using a single concentration measurement taken at a specific time after dosing. Similar to the two-level trapezoidal method (& thereby sharing many of their pros and cons), this method relies on established population pharmacokinetic equations to estimate the AUC and thereby oversimplifies true drug exposure.
Bayesian Method
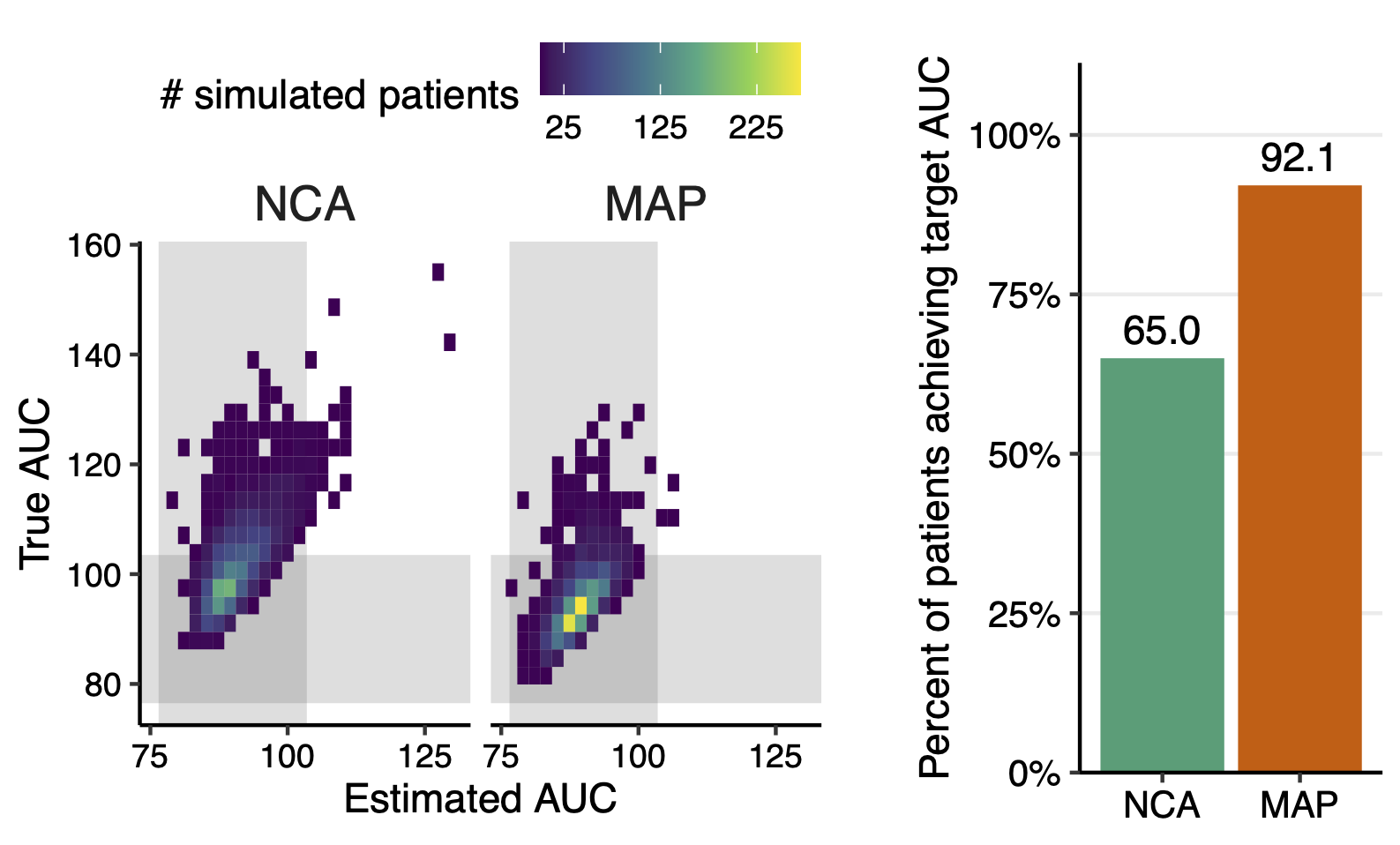
In contrast to the two-level trapezoidal method, Bayesian MIPD uses mathematical modeling to estimate AUC based on a combination of population kinetics, observed drug concentrations, and individual patient characteristics. These calculations are more comprehensive and complex, and require use of either online calculators or software programs, some of which can integrate with electronic health records. This method offers a more tailored approach, accounting for factors like renal function, weight, and age. By continuously updating estimates with new data, Bayesian modeling can adapt to changes in a patient's condition, potentially improving dosing accuracy and patient outcomes.
For this reason, among others, the Bayesian method is considered the preferred approach in the clinical practice guidelines:
“ The preferred approach to monitor AUC involves the use of Bayesian software programs, embedded with a PK model based on richly sampled vancomycin data as the Bayesian prior, to optimize the delivery of vancomycin. ”
Online “Bayesian” Calculators
Several free online tools (ClinCalc, GlobalRPh, VancoPK) are available that allege use of Bayesian principles to estimate vancomycin AUC. These calculators typically require input parameters such as patient demographics, renal function, and observed drug concentrations. While convenient and accessible, they are often limited in their scope and utility.
Many of these tools use pharmacokinetic models that have not been thoroughly validated, or may even perform poorly compared to other available models. Additionally, many calculators are unable to interpret multiple drug levels, or interpret inconsistent dosing histories, or account for dynamic changes in patient status. These systems also lack robust infrastructure, and so are unable to store data for future use, cannot integrate with electronic health records (EHRs), offer no user support, and have no guarantees of their accuracy. Compared to use of the trapezoidal method, however, use of a Bayesian method additionally provides more flexibility in sample timing and number of samples needed for AUC estimation.
| ✅ Pros | ⛔ Cons |
|---|---|
|
Accessibility: Free calculators are easily accessible online, making them convenient for healthcare professionals to use. |
Not truly “Bayesian": While many free vancomycin calculators claim to use Bayesian forecasting, they often fall short of fully implementing Bayes's Theorem. True Bayesian methods involve continuously updating PK estimates with new information. However, these calculators typically lack the flexibility to adapt to new data and iteratively refine their predictions resulting in less precise estimations. |
|
Simplified Interface: Free calculators often have simple interfaces, making them easy to use without requiring extensive training or expertise. |
Limited Validation & Inaccuracy: Online calculators often lack extensive validation for clinical use, making their accuracy and reliability questionable compared to commercial software. Due to variability in the quality of these calculators and their algorithms, there is a risk of inaccurate AUC estimation, which can lead to suboptimal dosing decisions. |
|
Cost-effective: As the name suggests, free calculators do not require any financial investment, which can be beneficial for healthcare settings with limited budgets. |
Lack of Support: Free calculators do not come with technical or clinical support in case of issues or questions regarding their use, and have no accountability to remain operational. |
|
Not HIPAA-compliant: Even without entering protected health information, inputting any patient data into non-secure platforms can pose risks and may often not be approved by hospital information security departments. |
|
|
Error-prone: As seen with the trapezoidal method, this method is also vulnerable to errors with manual entry of data. |
Model-Informed Precision Dosing Software
For institutions seeking a comprehensive approach to drug dosing optimization, sophisticated software solutions offer advanced Bayesian modeling capabilities with the potential for integration into EHR systems, analytics platforms, continuous improvement, and are often backed by readily-available clinician expertise.
 These software platforms typically provide robust features for data input, including real-time drug concentration monitoring and automated dose adjustment suggestions. By leveraging patient-specific data and advanced algorithms, these systems can proactively adapt dosing regimens to changing clinical conditions, improving both efficacy and safety. This adaptability is crucial because patient responses to drug therapy can evolve due to factors like changes in renal or hepatic function or fluctuations in disease severity. The ability to proactively adjust dosing ensures optimized, tailored therapy, enhancing efficacy and minimizing adverse events, ultimately supporting positive patient outcomes and safety.
These software platforms typically provide robust features for data input, including real-time drug concentration monitoring and automated dose adjustment suggestions. By leveraging patient-specific data and advanced algorithms, these systems can proactively adapt dosing regimens to changing clinical conditions, improving both efficacy and safety. This adaptability is crucial because patient responses to drug therapy can evolve due to factors like changes in renal or hepatic function or fluctuations in disease severity. The ability to proactively adjust dosing ensures optimized, tailored therapy, enhancing efficacy and minimizing adverse events, ultimately supporting positive patient outcomes and safety.
| ✅ Pros | ⛔ Cons |
|---|---|
|
Advanced Features: Bayesian MIPD software typically offers a wide range of features, including a broad set of population pharmacokinetic models, as well as individualized & real-time dosing recommendations. |
Costs: Bayesian MIPD software typically requires a financial investment. However, this can be offset by perceived return on investment as MIPD platforms are well-positioned to provide long-term financial benefits and overall net positive investment. |
|
EHR Integration: Some MIPD solutions provide the option to integrate into a hospital’s EHR to directly retrieve relevant medication, lab, and patient data. This decreases the rate of error seen with manual data entry, as well as decreases the time pharmacists spend evaluating a patient. |
Learning Curve: Using sophisticated software may require some additional training and familiarization, which could be time-consuming for healthcare professionals. While advanced software tools enable more sophisticated calculations to be performed at the click of a button, this also means that it can be a steeper learning curve for users to understand how the outputs are generated. |
|
Customization: Users can tailor the software to specific patient populations or clinical scenarios, addressing the unique needs and workflows of different healthcare institutions. |
|
|
Support: Commercial software solutions usually come with dedicated technical & clinical support, which can be invaluable for troubleshooting issues and optimizing software use. |
|
|
Validation and Compliance: Established commercial software solutions are likely to have undergone rigorous validation processes and comply with regulatory standards, instilling confidence in their accuracy and reliability. |
|
|
Adaptability and Evolution: Bayesian MIPD software, coupled with a data science team, offers the capability for continuous learning and adaptation. By analyzing real-world data and patient outcomes, the software can refine existing population pharmacokinetic models or develop new ones, leading to improved predictive capabilities over time. |
|
|
Analytics: Commercial software solutions are often coupled with analytic tools that can easily query real-time metrics related to the PK and clinical outcomes. |
Conclusion
The shift towards AUC monitoring represents a significant advancement in optimizing vancomycin therapy, aiming for greater precision and improved patient outcomes. While both the trapezoidal rule and Bayesian approaches offer avenues for estimating AUC, each method presents its own set of advantages and limitations. Clinicians must weigh these factors carefully, considering factors such as resource availability, patient population characteristics, and clinical expertise. Ultimately, the goal remains the same: delivering effective and safe antibiotic therapy tailored to the individual patient.
Want to learn more about AUC estimation and Bayesian modeling for vancomycin and other anti-infectives? Click below to learn more about our core infectious diseases bundle!