
The efficacy and toxicity of many drugs are linked to drug exposure quantified by the area under the concentration-time curve (AUC). For fixed regimen drugs with high inter-individual and intra-individual variability like busulfan, there are two main approaches for estimating AUC: non-compartmental analysis (NCA) and model-based methods, including Bayesian approaches.
These approaches operate under very different statistical methods, which has important implications for how they should be implemented into clinical practice. For example, NCA requires dense sampling and is more sensitive to sample timing, while Bayesian methods require a sufficiently descriptive model to estimate patient pharmacokinetics (PK).
To better understand the implications of the differences between these approaches and to guide clinical decision-making, we used a combination of retrospective analysis, simulation, and prospective analysis, using busulfan as a clinically relevant case study. We found that although both methods tend to produce very similar AUC estimates, maximum a posteriori (MAP) Bayesian-guided dose adaptation was more likely to achieve target AUC exposure. But before we get into these results, let’s do a quick review of how these two methods differ.
A practical introduction to non-compartmental analysis and MAP Bayesian estimation
Below, Figure 1 shows an example patient who received one dose of busulfan infused over 3 hours (grey shaded region) and then provided eight serum samples collected between 20 minutes and eight hours post-infusion.
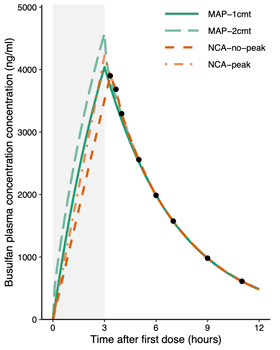
Figure 1: An example patient dosed with busulfan. Grey region indicates the infusion period, black circles indicate measured drug concentrations. Lines indicate concentration-time curves produced by MAP Bayesian (MAP) or non-compartmental analysis (NCA) methods. Reproduced from Hughes (2024) J PKPD.
NCA (orange lines) uses a log-linear graphical method to calculate the area under the measured concentration-time points. Or, in other words, a logarithmic decay is drawn between each measured concentration, and the infusion phase is modeled as a linear increase in concentration. Unsampled regions of the curve are estimated using linear regression to determine an average rate of elimination, and the exponential curve is extrapolated to the next dose and optionally to the end of infusion (“NCA-peak” versus “NCA-no-peak”). This method does not assume a particular number of drug distribution compartments, but it does assume a linear rise in concentration during infusion and first-order exponential decay between points. For extrapolated regions of the curve, NCA assumes that the unsampled regions of the curve follow the shape of the sampled regions of the curve, i.e., that the elimination rate characterizing first-order exponential decay remains constant over that time period. These considerations are summarized in Table 1.
For MAP Bayesian estimation (green lines), the most likely set of PK parameters for the patient is estimated, and those PK parameters are used to simulate a concentration-time curve. MAP Bayesian estimation requires a population PK model (which acts as a Bayesian prior), and the choice of model impacts the shape of the curve and the individual PK parameters estimated. For example, the difference in concentration-time curves between a one-compartment model and a two-compartment model are shown in Figure 1.
Something that might stand out in Figure 1 is that all four concentration-time curves are very similar during the elimination phase, but differ quite a bit during the (typically unsampled) infusion period. In particular, NCA assumes a linear rise in concentration during infusion, while the model-based methods assume a non-linear increase (due to the body already beginning to clear drug during infusion).
As summarized in Table 1, the differences between these methods impact clinical protocol design. Because NCA interpolates between points and extrapolates lines of best fit for unsampled regions, it requires dense sampling, and for as much of the concentration-time curve to be sampled as possible. In contrast, because Bayesian approaches balance data and the Bayesian prior to determine what a likely concentration-time curve would be, these approaches tend to be less sensitive to sample timing and can handle limited sampling strategies. Model-based methods also allow adjusting initial doses based on the patient covariates, while NCA requires weight-normalized or body surface area (BSA)-normalized dosing for initial doses.
Table 1: Comparison of non-compartmental analysis (NCA) with log-linear kinetics and model-based estimation using MAP Bayesian estimation of individual pharmacokinetic parameters.
| NCA (log-linear) | Bayesian (model-based) | |
| Assumptions |
|
|
| Sample requirement |
|
|
| Initial dose individualization |
|
|
| Post-TDM dose adjustments | Ratio of dose to estimated AUC is used to adjust dosing for the remainder of the treatment course | Patient PK parameters are estimated and used to simulate AUC given a particular dose, allowing for time-dependent factors like drug-related changes in clearance |
| Software requirement | Third-party software typically required to perform calculations | Third-party software typically required to perform calculations |
We’ve seen that there are a number of differences in how these two methods go about estimating AUC, but how do these AUC estimates vary by the numbers?
Difference in AUC estimation between NCA and MAP Bayesian estimation: A retrospective analysis of busulfan patients
In a recent collaboration with the University of California, San Francisco (UCSF) published in the Journal of Pharmacokinetics and Pharmacodynamics, we collected a data set of 246 patients treated with busulfan and who provided 2455 drug concentrations. We retrospectively calculated AUC for each dosing interval using NCA (with or without peak extension) or MAP Bayesian estimation (with a one-compartment or two-compartment model). All four methods showed good agreement with each other (Figure 2, Figure 3), although NCA methods tended to underestimate AUC relative to the MAP Bayesian approaches, consistent with the curve differences visible in Figure 1. On average, we would expect the two methods to differ by 5-13% for a given dosing interval, and so we would expect doses calculated according to these two methods to vary similarly.

Figure 2: Bland–Altman plots illustrating the agreement between different AUC estimation methods. Each data point represents an AUC estimate for a single dosing interval using the corresponding method. The dashed lines indicate the mean difference and the limits of agreement (mean difference ± 1.96 standard deviations). Adapted from Hughes (2024) J PKPD.

Figure 3: Correlation coefficient showing the strength of correlation between AUC estimates for each dosing interval. Adapted from Hughes (2024) J PKPD.
It’s important to remember that both of these methods estimate AUC, and for real world patients, we don’t know what their AUC truly was. To understand how accurately these methods estimate true AUC, we performed a simulation study.
How do differences in busulfan AUC estimation impact dose adjustment and target attainment: A simulated dose adaptation trial
Simulation allows us to see how well an AUC estimation method approaches the “true” AUC. For our simulation study, we created a set of digital patients who had the inter-patient and intra-patient variability described by the two-compartment busulfan population PK model published by McCune et al. (2015). We then used either NCA or MAP Bayesian estimation with the one-compartment PK model published by Shukla et al. (2020) to estimate AUC and adjust doses. We chose this experimental design to create a mismatch between the models used to simulate patient PK and estimate PK, since in the real world we will always have some degree of model misspecification. For a complete description of our methods and results, see our paper in the Journal of Pharmacokinetics and Pharmacodynamics.
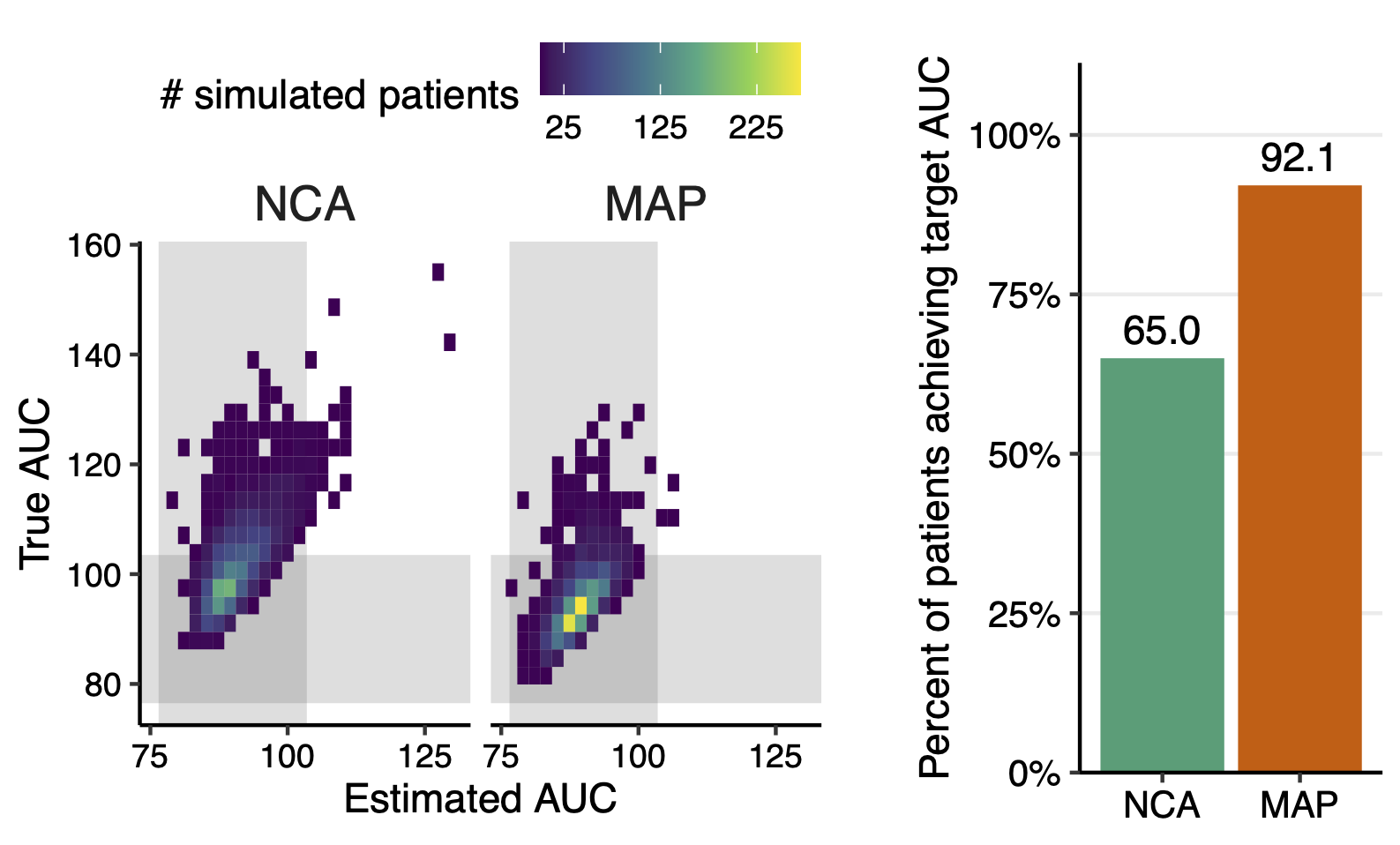
We found that simulated patients whose doses were adjusted according to NCA achieved an estimated cumulative AUC within the target range 98.7% of the time, while their true AUC was only in the target range 65% of the time. Patients treated according to MAP Bayesian estimates were also similarly confidently thought to be on target (99.9% estimated target attainment), however their true target attainment was much higher than for patients dosed according to NCA, at 92.1% (see Figure 4).

Figure 4: Comparison of NCA and MAP Bayesian estimation for dose adjustment in a simulated trial. (a) Comparison of true versus estimated AUC for each method, with shaded regions representing the target range (90 mg·h/L ± 15%). (b) Proportion of simulated patients achieving a true cumulative AUC within 15% of the target. Reproduced from Hughes (2024) J PKPD..
We looked into what the causes of these different rates of target attainment could be, and identified three main contributors:
- Assumptions about AUC during infusion: The differences in how model-based methods and NCA handle infusion create very different curve shapes (see Figure 1), translating to very different AUC estimates, as shown in Figure 5. For the long infusions typical of once-daily busulfan, this can make up a significant amount of the total AUC.

Figure 5: Comparison of estimated versus true AUC for NCA versus MAP Bayesian estimation during infusion, after infusion, and across the full dosing interval. m Hughes (2024) J PKPD..
- Handling time-dependent changes in drug PK: Busulfan clearance is reported to decrease during therapy. Model-based methods can anticipate these changes, leading to less drastic dose adjustments. In contrast, NCA does not consider day-to-day changes in patient PK, resulting in overcompensation for day 1 and under-dosing on day 2, as shown in Figure 6.

Figure 6: Comparison of AUCs by dose according to the two estimation methods. Reproduced from Hughes (2024) J PKPD..
- Accumulation of information: NCA only considers information collected during the most recent dosing interval, while MAP Bayesian estimates include information from all dosing intervals to get a better understanding of patient PK over the course of therapy. When we re-ran the experiment such that MAP Bayesian estimation only had access to information from one dosing interval at a time, we saw a decrease in target attainment by 1.8% (see Figure 7 versus Figure 4).

Figure 7: Estimated versus true target attainment when MAP Bayesian estimation only considers samples from the most recent day of dosing, more closely approximating NCA. Reproduced from Hughes (2024) J PKPD..
Simulation helps us see how differences in statistical methods impact patient care by allowing “trials” that would be impossible or inadvisable in real patients, however the best test is always comparison in real patients. So how do these two methods stack up in a real clinical setting?
Target Attainment in patients treated according to NCA versus MAP Bayesian estimation: A prospective study
In this collaboration with UCSF, 188 pediatric and young adult patients were treated with busulfan according to three approaches:
- For Cohort A, initial doses were selected according to conventional dosing guidelines, and NCA was used for AUC estimation and dose adjustment.
- For Cohort B, initial doses were selected according to an older population PK model, and NCA was used for AUC estimation and dose adjustment.
- For Cohort C, initial doses were selected according to an updated PK model, and doses were adjusted using MAP Bayesian estimation.
We found that target attainment was highest in the cohort treated according to MAP Bayesian estimation (Cohort C: 100%) compared to the cohorts treated according to NCA (Cohort A: 66%, Cohort B: 88%), as shown in Figure 8.

Figure 8: Difference in target attainment according to the three study arms. Cohort A and Cohort B: dose adjustment using NCA. Cohort C: dose adjustment using MAP Bayesian estimation. Reproduced from Shukla (2020) Front. Pharmacol.
Conclusions: How can I implement precision dosing at my organization?
We’ve seen that algorithmic differences between NCA and MAP Bayesian estimation have significant impacts on AUC estimation and achieving target drug exposures. NCA, while less accurate for dose personalization, remains an essential tool in clinical pharmacology. Its lack of dependency on model assumptions makes it useful for regulatory reporting and for patients not represented in population models. While model-based methods require a sufficiently descriptive model, MAP Bayesian-guided dose adjustment results in better target attainment and reduced variability in dosing, and allows for limited sampling schemes.
Implementing MAP approaches in clinical settings represents a significant step forward in modernizing precision dosing practices. For clinicians and hospital pharmacists, this shift presents an opportunity to embrace more accurate and patient-centered dosing strategies, ultimately advancing the standard of care.
Interested in implementing either NCA or MAP Bayesian estimation at your institution? Learn more about our MIPD Drug Modules for BMT conditioning below!
